The Paris endoscope classification is the Japanese endoscopic classification of superficial neoplastic lesions of the GI tract. Neoplastic lesions, which are the abnormal growth of tissues, in the digestive tract are called “superficial” if the lesion looks like small cancer or a noninvasive neoplastic lesion (including dysplasia, which is the abnormal growth of cells in an organ, and adenoma, which is non-cancerous tumours).
6 Types of lesions
The Paris endoscope classification has 6 types including the following:
type 0 – superficial polypoid, flat/depressed, or excavated tumors
type 1 – polypoid carcinomas, usually attached on a wide base
type 2 – ulcerated carcinomas with sharply demarcated and raised margins
type 3 – ulcerated, infiltrating carcinomas without definite limits
type 4 – nonulcerated, diffusely infiltrating carcinomas
type 5 – unclassifiable advanced carcinomas
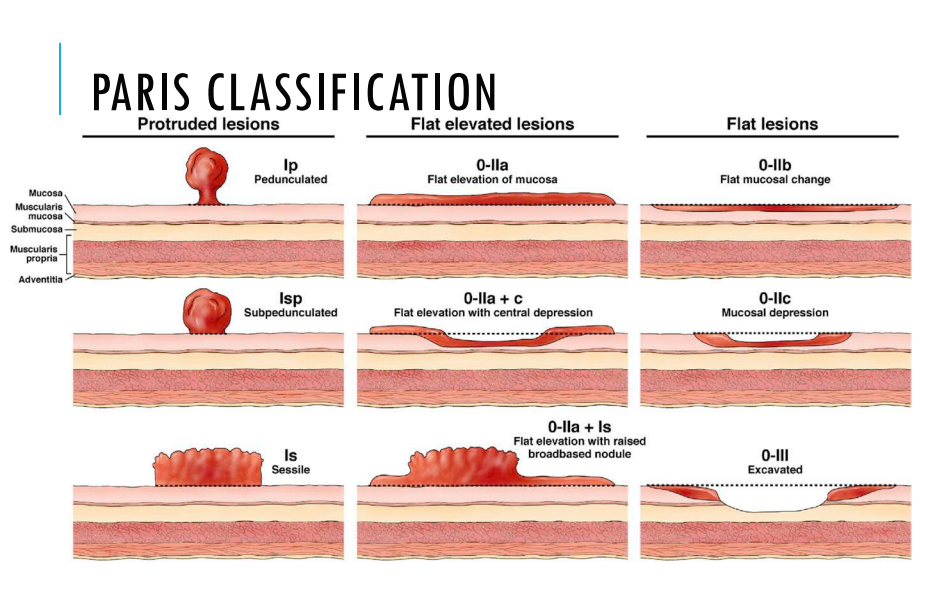
Type 0 with its subtypes adapted to endoscopic appearance, which includes polypoid (Ip and Is), non-polypoid (IIa, IIb, and II c), non-polypoid and excavated (III) as shown in the image below:
Pros and Cons of this classification method
Cons
Many Western specialist indicated that this classification is too complex for practical use, and here are some suggested draw back of this method:
- Most type 0-II small colorectal lesions are non-cancerous or low-grade intraepithelial neoplasia (abnormal cells found on the surface of or in the tissue that lines the organ)
- Most type 0-II lesions have a low potential for invasion.
- Most lesions are detectable without chromoendoscopy (the process of applying dye to a lesion)
- After a colonoscopy “negative for cancer,” the number of cancers detected during a 5-year follow-up is small. In a 5.9 years follow-up study only 0.35% of the group were detected with cancer
- The benefit of detecting such lesions to save lives at a cost that is acceptable per year of life saved is unproven
Pros
- The routine use of chromoendoscopy may have a major educational role in improving the detection of small and advanced lesions during standard endoscopy
- 5.2% of patient from a different study group with confirmed cancer had one or more negative colonoscopies during the previous 5 years
- 2 European randomized trials show a high proportion of colorectal cancers detected in the 2-year interval after a “negative” test. Small and evolving depressed (or non-depressed) neoplastic lesions could explain this result.
Overall, the reliability of Paris classification is moderate to good. Training on this classification or its revision and use of technology such as NBI may improve not only reliability and agreement but also accuracy.
Reference
NCI Dictionary of Cancer terms. National Cancer Institute. (n.d.). Retrieved June 21, 2022, from https://www.cancer.gov/publications/dictionaries/cancer-terms/def/intraepithelial
NCI Dictionary of Cancer terms. National Cancer Institute. (n.d.). Retrieved June 21, 2022, from https://www.cancer.gov/publications/dictionaries/cancer-terms/def/neoplasm
Participants in the Paris Workshop. (2002). The Paris Endoscopic Classification of Superficial Neoplastic Lesions: Esophagus, Stomach, and Colon. https://doi.org/https://doi.org/10.1016/S0016-5107(03)02159-X
Ribeiro, H., Libânio, D., Castro, R., Ferreira, A., Barreiro, P., Boal Carvalho, P., Capela, T., Pimentel-Nunes, P., Santos, C., & Dinis-Ribeiro, M. (2019, May). Reliability of Paris classification for superficial neoplastic gastric lesions improves with training and narrow band imaging. Endoscopy international open. Retrieved June 21, 2022, from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6497497/