Resection in the medical field refers to the procedure of removing tissue or part or all of an organ, and resection endoscopy usually involves removing abnormal tissues using an endoscope. According to ACG Case Reports Journal: January 2021, resection endoscopy, which was pioneered in Asia, is currently spreading swiftly within western countries. It is highly efficient in preventing cancer and its spreading, as it provides a method that can spare the cost, morbidity, and mortality of surgery to remove precancerous and early-stage cancer tissues.
1. Endoscopic Mucosal Resection (EMR)
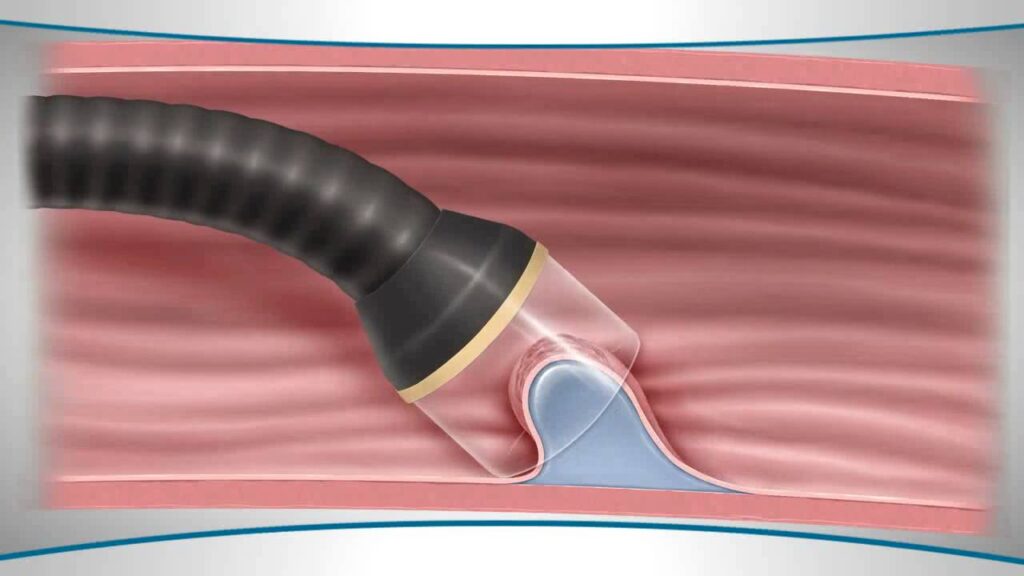
EMR is an outpatient procedure in which physicians remove tumours just beneath the gastrointestinal (GI) wall without surgery. EMR is most effective for tumours that have not yet reached deeper layers of the GI wall and are larger than 2 centimetres. EMR can treat conditions such as Barrett’s esophagus, precancerous or superficial cancerous tumours such as gastric or small bowel lesions (areas of abnormal tissue) and also early-stage esophageal cancer or colon cancer.
2. Endoscopic Submucosal Dissection (ESD)
ESD is an outpatient procedure to remove deep tumours from the GI tract. In some cases, ESD is a more effective option than EMR for removing growths or tumours. ESD may treat Barrett’s esophagus, early-stage cancerous tumours or colon polyps, tumours of the esophagus, stomach or colon that have not yet entered the deeper layer of the GI wall, with minimal or no risk of cancer spreading, and staging of cancer (determining the cancer level) to develop treatment plans.
3. Endoscopic Full Thickness Resection (EFTR)
EFTR is an outpatient procedure to remove growths deep in the wall of the gastrointestinal (GI) tract. EFTR is very effective for removing tumours located deep in the GI wall. Because of the location of these growths, other procedures could cause complications, such as tearing or perforation of tissue. It is more effective than EMR or ESD for safely removing tumours in the shallow layers of the GI wall that adhere to the muscle layer. In addition to deep tumours, physicians may use EFTR for GI bleeding, postsurgical complications such as a perforation (tear). stomach, small bowel or colon polyp removal (polypectomy), and closing holes or openings between organs or tissues (chronic fistula).